
Oat Intake and Risk of Type 2 Diabetes, Cardiovascular Disease and All-Cause Mortality: A Systematic Review and Meta-Analysis

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
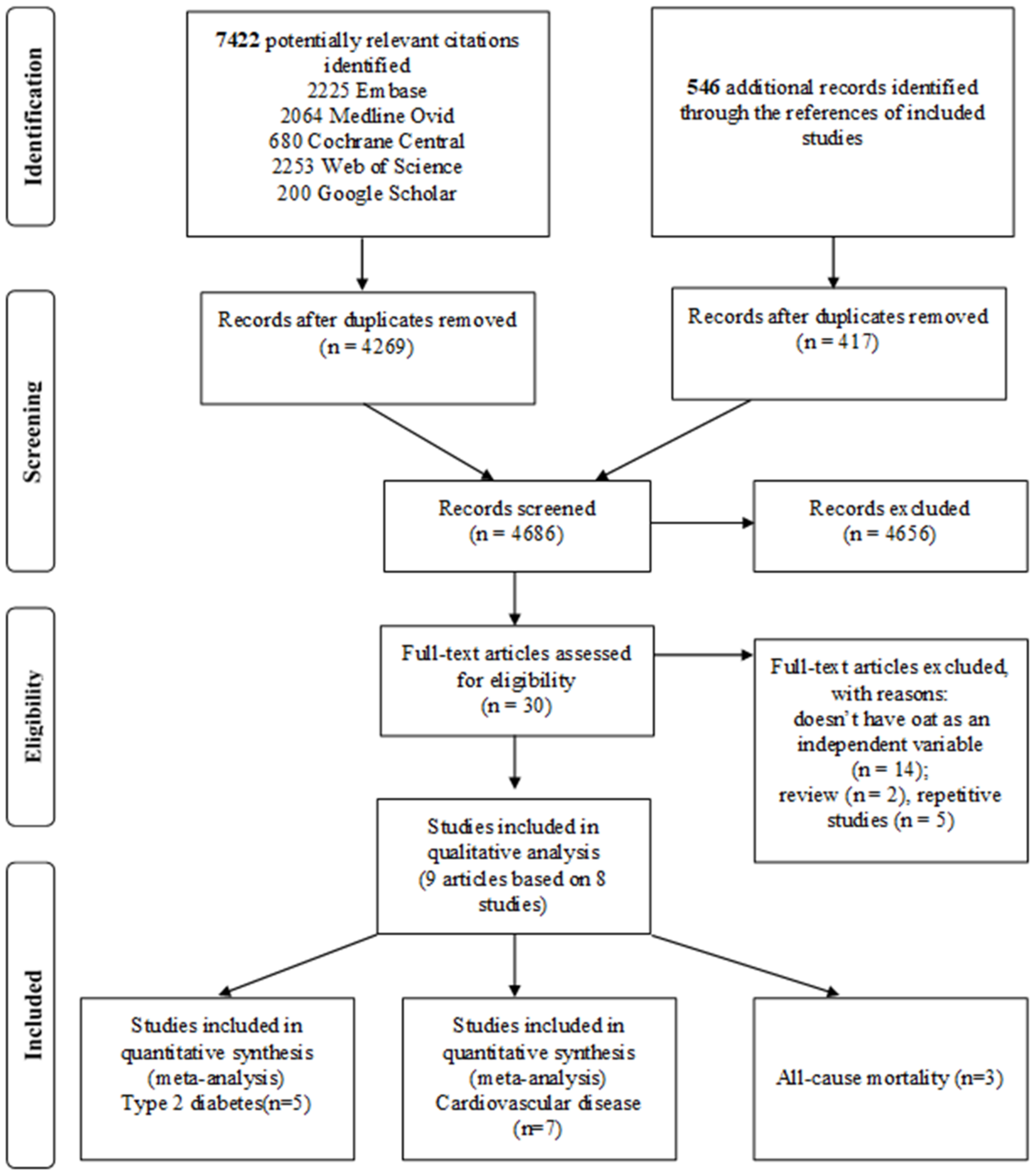
3.1. Study Identification and Selection
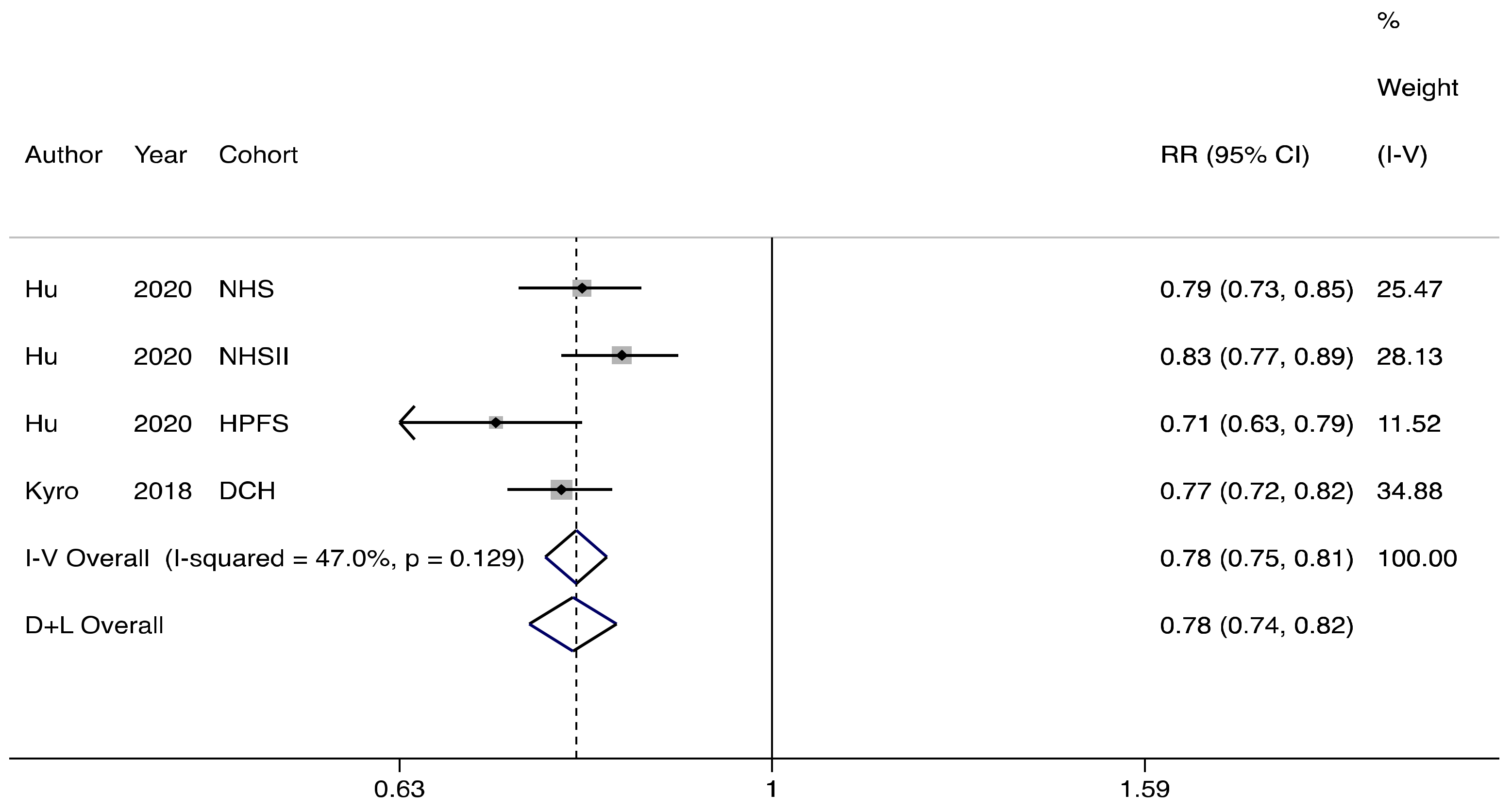
3.2. Association between Oat Consumption and Risk of Type 2 Diabetes
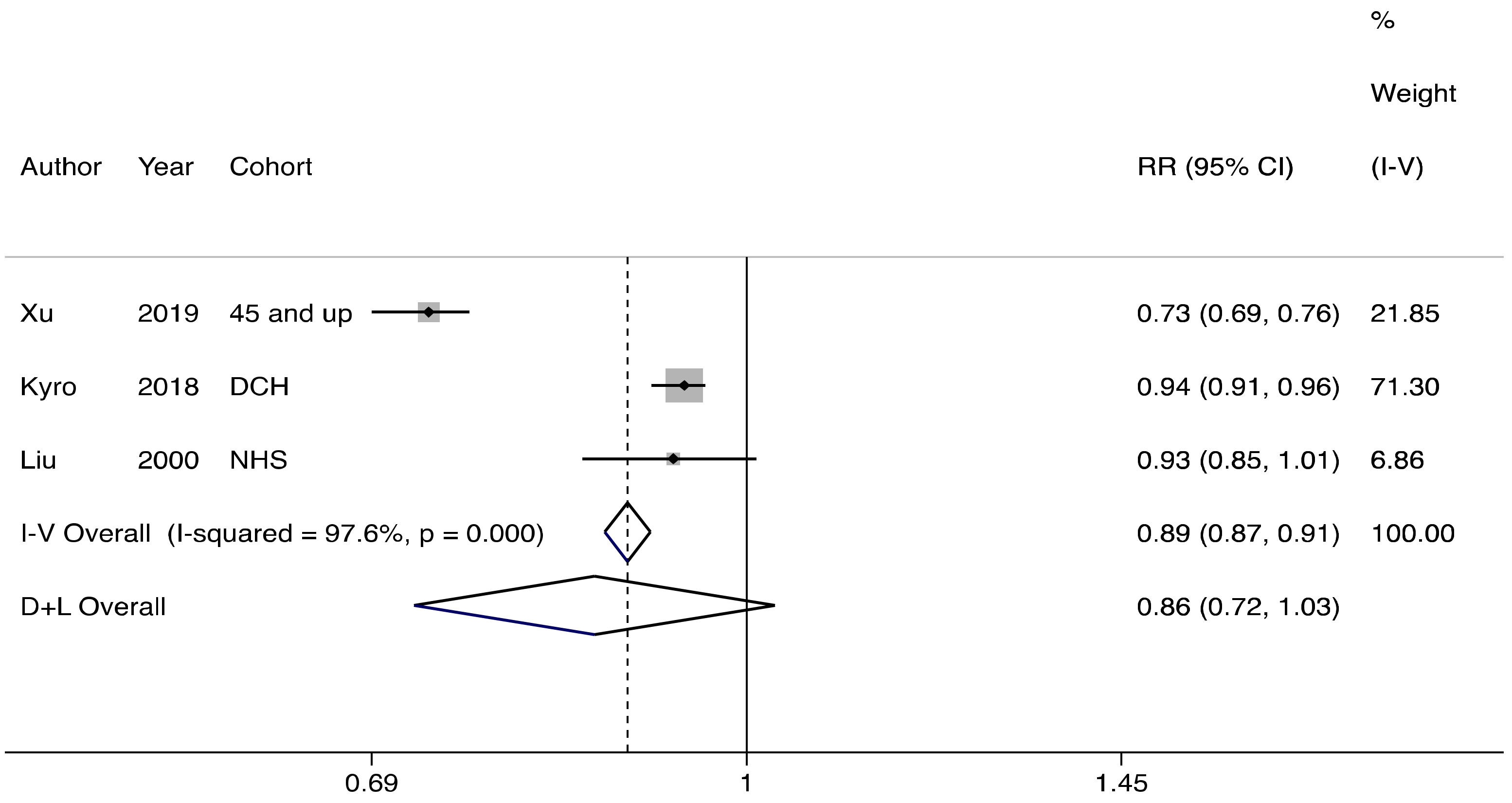
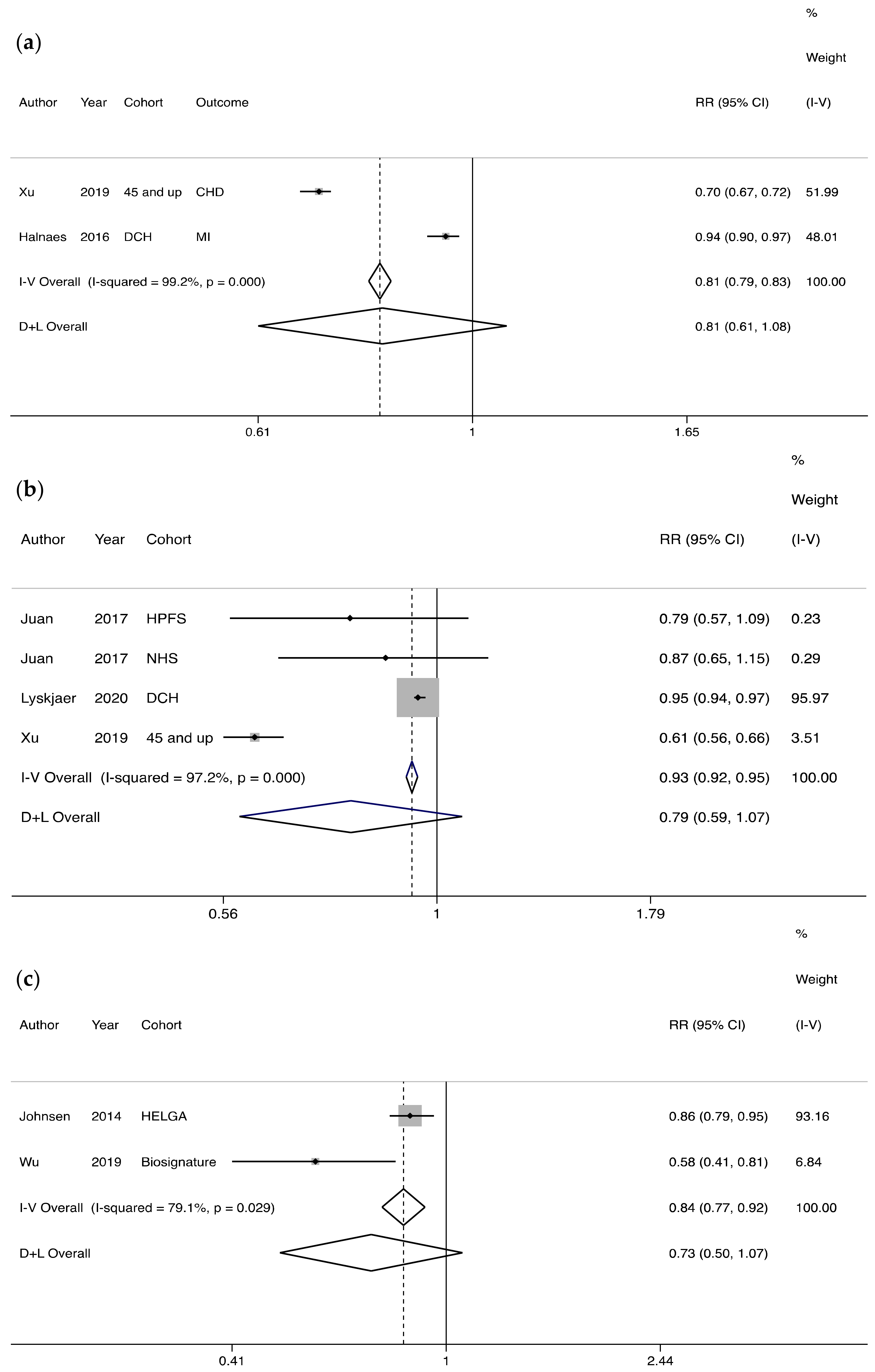
3.3. Association between Oat Consumption and Risk of Cardiovascular Disease
3.4. Association between Oat Consumption and All-Cause Mortality
3.5. Study Quality
3.6. Sensitivity Analysis
4. Discussion
4.1. Principal Findings
4.2. Comparison with Other Studies
4.3. Potential Underlying Mechanisms
4.4. Strengths and Limitations of the Study
4.5. Implications for Clinicians and Policy Makers
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A. Full Search Strategy per Database
- Embase.com
- Medline (Ovid)
- Cochrane Library (Wiley)
- Web of Science Core Collection
- Google scholar (first 200 results, out of 23′000)
References
- FAOSTAT. FAOSTAT. 2019. Available online: http://www.fao.org/faostat/en/#data/QC (accessed on 8 October 2020).
- Raguindin, P.F.; Itodo, O.A.; Stoyanov, J.; Dejanovic, G.M.; Gamba, M.; Asllanaj, E.; Minder, B.; Bussler, W.; Metzger, B.; Muka, T.; et al. A systematic review of phytochemicals in oat and buckwheat. Food Chem. 2021, 338, 127982. [Google Scholar] [CrossRef]
- Meydani, M. Potential health benefits of avenanthramides of oats. Nutr. Rev. 2009, 67, 731–735. [Google Scholar] [CrossRef]
- Von Noorden, C. Hafercuren bei schwerem diabetes mellitus. Klin Wochenschr 1903, 36, 817–821. [Google Scholar]
- Hou, Q.; Li, Y.; Li, L.; Cheng, G.; Sun, X.; Li, S.; Tian, H. The metabolic effects of oats intake in patients with type 2 diabetes: A systematic review and meta-analysis. Nutrients 2015, 7, 10369–10387. [Google Scholar] [CrossRef] [Green Version]
- Nazare, J.A.; Normand, S.; Oste Triantafyllou, A.; Brac de la Perrière, A.; Desage, M.; Laville, M. Modulation of the postprandial phase by beta-glucan in overweight subjects: Effects on glucose and insulin kinetics. Mol. Nutr. Food Res. 2009, 53, 361–369. [Google Scholar] [CrossRef]
- Jenkins, A.L.; Jenkins, D.J.A.; Zdravkovic, U.; Würsch, P.; Vuksan, V. Depression of the glycemic index by high levels of beta-glucan fiber in two functional foods tested in type 2 diabetes. Eur. J. Clin. Nutr. 2002, 56, 622–628. [Google Scholar] [CrossRef]
- Tapola, N.; Karvonen, H.; Niskanen, L.; Mikola, M.; Sarkkinen, E. Glycemic responses of oat bran products in type 2 diabetic patients. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 255–261. [Google Scholar] [CrossRef]
- Whitehead, A.; Beck, E.J.; Tosh, S.; Wolever, T.M. Cholesterol-lowering effects of oat β-glucan: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2014, 100, 1413–1421. [Google Scholar] [CrossRef] [Green Version]
- Nie, L.; Wise, M.L.; Peterson, D.M.; Meydani, M. Avenanthramide, a polyphenol from oats, inhibits vascular smooth muscle cell proliferation and enhances nitric oxide production. Atherosclerosis 2006, 186, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Sur, R.; Nigam, A.; Grote, D.; Liebel, F.; Southall, M.D. Avenanthramides, polyphenols from oats, exhibit anti-inflammatory and anti-itch activity. Arch. Dermatol. Res. 2008, 300, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Beck, E.J.; Tapsell, L.C.; Batterham, M.J.; Tosh, S.M.; Huang, X.F. Oat beta-glucan supplementation does not enhance the effectiveness of an energy-restricted diet in overweight women. Br. J. Nutr. 2010, 103, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Keenan, J.M.; Pins, J.J.; Frazel, C.; Moran, A.; Turnquist, L. Oat ingestion reduces systolic and diastolic blood pressure in patients with mild or borderline hypertension: A pilot trial. J. Fam. Pract. 2002, 51, 369. [Google Scholar]
- Olsen, A.; Egeberg, R.; Halkjær, J.; Christensen, J.; Overvad, K.; Tjønneland, A. Healthy Aspects of the Nordic Diet Are Related to Lower Total Mortality. J. Nutr. 2011, 141, 639–644. [Google Scholar] [CrossRef]
- McGeoch, S.C.; Johnstone, A.; Lobley, G.E.; Adamson, J.; Hickson, K.; Holtrop, G.; Fyfe, C.; Clark, L.F.; Pearson, D.W.M.; Abraham, P.; et al. A randomized crossover study to assess the effect of an oat-rich diet on glycaemic control, plasma lipids and postprandial glycaemia, inflammation and oxidative stress in Type 2 diabetes. Diabet. Med. 2013, 30, 1314–1323. [Google Scholar] [CrossRef] [Green Version]
- Cugnet-Anceau, C.; Nazare, J.A.; Biorklund, M.; Le Coquil, E.; Sassolas, A.; Sothier, M.; Holm, J.; Landin-Olsson, M.; Önning, G.; Laville, M.; et al. A controlled study of consumption of beta-glucan-enriched soups for 2 months by type 2 diabetic free-living subjects. Br. J. Nutr. 2010, 103, 422–428. [Google Scholar] [CrossRef] [Green Version]
- Muka, T.; Glisic, M.; Milic, J.; Verhoog, S.; Bohlius, J.; Bramer, W.; Chowdhury, R.; Franco, O.H. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur. J. Epidemiol. 2019, 35, 49–60. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 July 2020).
- Schünemann, H.B.J.; Guyatt, G.; Oxman, A. GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 23 July 2021).
- Grant, R.L. Converting an odds ratio to a range of plausible relative risks for better communication of research findings. BMJ 2014, 348, f7450. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.-R.; Leu, H.-B.; Yin, W.-H.; Tseng, W.-K.; Wu, Y.-W.; Lin, T.-H.; Yeh, H.-I.; Chang, K.-C.; Wang, J.-H.; Wu, C.-C.; et al. The benefit of secondary prevention with oat fiber in reducing future cardiovascular event among CAD patients after coronary intervention. Sci. Rep. 2019, 9, 3091. [Google Scholar] [CrossRef]
- Xu, X.; Parker, D.; Inglis, S.C.; Byles, J. Can regular long-term breakfast cereals consumption benefits lower cardiovascular diseases and diabetes risk? A longitudinal population-based study. Ann. Epidemiol. 2019, 37, 43–50.e3. [Google Scholar] [CrossRef]
- Johnsen, N.F.; Frederiksen, K.; Christensen, J.; Skeie, G.; Lund, E.; Landberg, R.; Johansson, I.; Nilsson, L.M.; Halkjær, J.; Olsen, A.; et al. Whole-grain products and whole-grain types are associated with lower all-cause and cause-specific mortality in the Scandinavian HELGA cohort. Br. J. Nutr. 2015, 114, 608–623. [Google Scholar] [CrossRef] [Green Version]
- Helnæs, A.; Kyrø, C.; Andersen, I.; Lacoppidan, S.; Overvad, K.; Christensen, J.; Tjønneland, A.; Olsen, A. Intake of whole grains is associated with lower risk of myocardial infarction: The Danish Diet, Cancer and Health Cohort. Am. J. Clin. Nutr. 2016, 103, 999–1007. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Ding, M.; Sampson, L.; Willett, W.C.; Manson, J.E.; Wang, M.; Rosner, B.; Hu, F.B.; Sun, Q. Intake of whole grain foods and risk of type 2 diabetes: Results from three prospective cohort studies. BMJ 2020, 370, m2206. [Google Scholar] [CrossRef]
- Juan, J.; Liu, G.; Willett, W.C.; Hu, F.B.; Rexrode, K.; Sun, Q. Whole Grain Consumption and Risk of Ischemic Stroke: Results from 2 Prospective Cohort Studies. Stroke 2017, 48, 3203–3209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyrø, C.; Tjønneland, A.; Overvad, K.; Olsen, A.; Landberg, R. Higher whole-grain intake is associated with lower risk of type 2 diabetes among middle-aged men and women: The danish diet, cancer, and health cohort. J. Nutr. 2018, 148, 1434–1444. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Manson, J.E.; Stampfer, M.J.; Hu, F.; Giovannucci, E.; Colditz, G.; Hennekens, C.H.; Willett, W.C. A prospective study of whole-grain intake and risk of type 2 diabetes mellitus in US women. Am. J. Public Health 2000, 90, 1409–1415. [Google Scholar] [PubMed] [Green Version]
- Lyskjær, L.; Overvad, K.; Tjonneland, A.; Dahm, C. Substitutions of Oatmeal and Breakfast Food Alternatives and the Rate of Stroke. Stroke 2020, 51, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lacoppidan, S.A.; Kyrø, C.; Loft, S.; Helnæs, A.; Christensen, J.; Hansen, C.P.; Dahm, C.C.; Overvad, K.; Tjønneland, A.; Olsen, A. Adherence to a healthy nordic food index is associated with a lower risk of type-2 diabetes—The danish diet, cancer and health cohort study. Nutrients 2015, 7, 8633–8644. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 241–284. [Google Scholar]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [Green Version]
- Hollænder, P.L.; Ross, A.B.; Kristensen, M. Whole-grain and blood lipid changes in apparently healthy adults: A systematic review and meta-analysis of randomized controlled studies. Am. J. Clin. Nutr. 2015, 102, 556–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajishafiee, M.; Saneei, P.; Benisi-Kohansal, S.; Esmaillzadeh, A. Cereal fibre intake and risk of mortality from all causes, CVD, cancer and inflammatory diseases: A systematic review and meta-analysis of prospective cohort studies. Br. J. Nutr. 2016, 116, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Vuksan, V.; Jenkins, A.L.; Rogovik, A.L.; Fairgrieve, C.D.; Jovanovski, E.; Leiter, L.A. Viscosity rather than quantity of dietary fibre predicts cholesterol-lowering effect in healthy individuals. Br. J. Nutr. 2011, 106, 1349–1352. [Google Scholar] [CrossRef] [Green Version]
- Yu, K.; Ke, M.-Y.; Li, W.-H.; Zhang, S.-Q.; Fang, X.-C. The impact of soluble dietary fibre on gastric emptying, postprandial blood glucose and insulin in patients with type 2 diabetes. Asia Pac. J. Clin. Nutr. 2014, 23, 210–218. [Google Scholar]
- Chen, J.-P.; Chen, G.C.; Wang, X.; Qin, L.; Bai, Y. Dietary Fiber and Metabolic Syndrome: A Meta-Analysis and Review of Related Mechanisms. Nutrients 2017, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, S.V.; Hannon, B.A.; An, R.; Holscher, H.D. Effects of isolated soluble fiber supplementation on body weight, glycemia, and insulinemia in adults with overweight and obesity: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2017, 106, 1514–1528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, C.E.; Greenwood, D.C.; Threapleton, D.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.E.; Gale, C.P.; Burley, V.J. Effects of dietary fibre type on blood pressure: A systematic review and meta-analysis of randomized controlled trials of healthy individuals. J. Hypertens. 2015, 33, 897–911. [Google Scholar] [CrossRef] [Green Version]
- El Khoury, D.; Cuda, C.; Luhovyy, B.L.; Anderson, G.H. Beta glucan: Health benefits in obesity and metabolic syndrome. J. Nutr. Metab. 2012, 2012, 851362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaremba, S.M.; Gow, I.F.; Drummond, S.; McCluskey, J.T.; Steinert, R.E. Effects of oat β-glucan consumption at breakfast on ad libitum eating, appetite, glycemia, insulinemia and GLP-1 concentrations in healthy subjects. Appetite 2018, 128, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Tabesh, F.; Sanei, H.; Jahangiri, M.; Momenizadeh, A.; Tabesh, E.; Pourmohammadi, K.; Sadeghi, M. The effects of beta-glucan rich oat bread on serum nitric oxide and vascular endothelial function in patients with hypercholesterolemia. BioMed Res. Int. 2014, 2014, 481904. [Google Scholar] [CrossRef] [PubMed]
- Croft, K.D. Dietary polyphenols: Antioxidants or not? Arch. Biochem. Biophys. 2016, 595, 120–124. [Google Scholar] [CrossRef] [Green Version]
- He, L.-X.; Zhao, J.; Huang, Y.-S.; Li, Y. The difference between oats and beta-glucan extract intake in the management of HbA1c, fasting glucose and insulin sensitivity: A meta-analysis of randomized controlled trials. Food Funct. 2016, 7, 1413–1428. [Google Scholar] [CrossRef]
- Beck, E.J.; Tapsell, L.C.; Batterham, M.J.; Tosh, S.M.; Huang, X.F. Increases in peptide Y-Y levels following oat beta-glucan ingestion are dose-dependent in overweight adults. Nutr. Res. 2009, 29, 705–709. [Google Scholar] [CrossRef] [Green Version]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [Green Version]
- Longo, V.D. Programmed longevity, youthspan, and juventology. Aging Cell 2018, 18, e12843. [Google Scholar] [CrossRef] [PubMed]
- Havrlentova, M.; Petrulakova, Z.; Burgarova, A.; Gago, F.; Hlinkova, A.; Šturdík, E. Cereal beta-glucans and their significance for the preparation of functional foods—A review. Czech J. Food Sci. 2018, 29, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Barnard, N.D.; Cohen, J.; Jenkins, D.J.; Turner-McGrievy, G.; Gloede, L.; Green, A.; Ferdowsian, H. A low-fat vegan diet and a conventional diabetes diet in the treatment of type 2 diabetes: A randomized, controlled, 74-wk clinical trial. Am. J. Clin. Nutr. 2009, 89, 1588S–1596S. [Google Scholar] [CrossRef]
- Silano, M.; Pozo, E.P.; Uberti, F.; Manferdelli, S.; Del Pinto, T.; Felli, C.; Budelli, A.; Vincentini, O.; Restani, P. Diversity of oat varieties in eliciting the early inflammatory events in celiac disease. Eur. J. Nutr. 2014, 53, 1177–1186. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Study Location | Cohort Name | No. of Individuals | Median Age (5th–95th Percentile) | Percentage of Males | Mean/Medium Follow up Time, Years | Oat Intake | Median Oat Intake in Population, g/day | Number of Events | Study Quality | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T2D | CVD | All-Cause Mortality | ||||||||||
| Helnaes (2016) [25] | Denmark | Danish Diet, Cancer, and Health cohort (DCH) | 54871 | all m 1: 25921: 55.0 (50.0–64.0) | 47.2 | 13.6 median | oatmeal | 1 | NA | 2329 | NA | 8 |
| cases m: 1676: 57.0 (51.0–64.0) | ||||||||||||
| all w 1: 28950: 56.0 (50.0–64.0) | ||||||||||||
| cases w: 653: 59.0 (51.0–64.0) | ||||||||||||
| Hu (2020) [26] | US | Nurses’ Health Study (NHS) | 69139 | mean 30 | 0 | 24 mean | oatmeal | NA | 9723 | NA | NA | 7 |
| Nurses’ Health Study II (NHSII) | 89120 | 0 | 6821 | |||||||||
| Health Professionals Follow-up Study (HPFS) | 36525 | 100 | 2085 | |||||||||
| Johnsen (2015) [24] | Scandinavian | HELGA 2 | 119518 | w: 51 (40–63) m: 54 (31–64) | 33 | NA | whole grain oats | 2 | NA | 298 women, 858 men died from CHD 3, 137 women, 143 men dies from stroke | 7839 | 7 |
| Norway | the Norwegian Women and Cancer Study | 37111 | 0 | 11.1 median | NA | 966 | ||||||
| Sweden | the Vasterbotten Intervention Programme cohort | 25551 | 48.3 | 14.2 median | NA | 1367 | ||||||
| Denmark | the Danish Diet Cancer and Health Study | 56865 | 47.6 | 11.9 median | NA | 5506 | ||||||
| Juan (2017) [27] | US | Health Professionals Follow-up Study | 42823 | mean (SD) 53.2(9.5) | 100 | 24 | oatmeal | NA | NA | NA | 908 | 7 |
| Nurses’ Health Study | 71750 | mean (SD) 50.1(7.1) | 0 | 26 | 1550 | |||||||
| Kyro (2018) [28] | Denmark | Diet, Cancer, and Health cohort | 55465 | 50–65 | 47.3 | 15 | whole grain oat, oatmeal | 1 | 7417 | NA | NA | 9 |
| Liu (2000) [29] | US | Nurses’ Health Study | 75521 | 38–63 mean | 0 | 10 | oatmeal | NA | 1879 | NA | NA | 7 |
| Lyskjaer (2020) [30] | Denmark | Diet, Cancer, and Health cohort | 55095 | 56.1(52.7–60.3) | 47.6 | 13.4 median | oatmeal | 0.7 | NA | 2260 | NA | 8 |
| Olsen (2011) [14] | Denmark | Diet, Cancer, and Health cohort | 57053 | 50–64 | 46.3 | 12 | oatmeal | 0.8 | NA | NA | 4126 | 9 |
| Xu (2019) [23] | Australia | 45 and Up Study | 142503 | 45–64y 37,626 all cases | NA | 3 | oat cereal | NA | 5283 | Heart disease 14148, stroke 2911 | NA | 5 |
| 65–80y 24,203 all cases | ||||||||||||
| >80 y 5967 | ||||||||||||
| Wu (2019) [22] | Taiwan | The Biosignature study | 1663 | mean ± SD nouse:65.26 ± 12.19 oat:68.82 ± 11.65 | 36.6 | mean 26.75 ± 8.11 months | oat fiber (oat bran, oat containing products) | NA | NA | 175 | N/A | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wehrli, F.; Taneri, P.E.; Bano, A.; Bally, L.; Blekkenhorst, L.C.; Bussler, W.; Metzger, B.; Minder, B.; Glisic, M.; Muka, T.; et al. Oat Intake and Risk of Type 2 Diabetes, Cardiovascular Disease and All-Cause Mortality: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2560. https://doi.org/10.3390/nu13082560
Wehrli F, Taneri PE, Bano A, Bally L, Blekkenhorst LC, Bussler W, Metzger B, Minder B, Glisic M, Muka T, et al. Oat Intake and Risk of Type 2 Diabetes, Cardiovascular Disease and All-Cause Mortality: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(8):2560. https://doi.org/10.3390/nu13082560
Chicago/Turabian StyleWehrli, Faina, Petek E. Taneri, Arjola Bano, Lia Bally, Lauren C. Blekkenhorst, Weston Bussler, Brandon Metzger, Beatrice Minder, Marija Glisic, Taulant Muka, and et al. 2021. "Oat Intake and Risk of Type 2 Diabetes, Cardiovascular Disease and All-Cause Mortality: A Systematic Review and Meta-Analysis" Nutrients 13, no. 8: 2560. https://doi.org/10.3390/nu13082560